Have you recently been feeling like your body just isn’t performing like it used to? Like you’re telling it to stay active, perform, and be able to lift, reach and bend but things keep popping, snapping, or shifting? Do you describe yourself as double-jointed or extra flexible? Or are you like me, and have a weird party trick like pulling your shoulders out of the socket on demand?
What was once a flexible body capable of playing sports and keeping up with friends, turned into constant ankle sprains and injuries in high school and early adulthood, and by 30-40 turns into an inescapable fatigue, joint pain, and a sudden inability of your joints to stay in place and follow your brain’s commands? For symptomatic hypermobile women, times around puberty and perimenopause can wreak havoc on our joint stability, mood, energy availability and our pain, and it’s not just hormonal. You’ve been able to be active without pain before, let me help you get back to that, it’s possible!

From “Party Tricks” to Pain
There is a wide spectrum of hypermobility, with many people only having flexible joints (aka asymptomatic hypermobility). However, another subset of bendy people have symptoms that interrupt “normal” physiologic functions as a result of a connective tissue disorder. Symptomatic hypermobile (S-hEDS) patients start having symptoms (dislocations, subluxations, autoimmune issues, dysautonomia, easy bruising) early in their teens, around 9-12 years old. You might remember having “party tricks” such as pulling joints out of place, calling yourself double-jointed, doing the splits, or palming the floor with ease. You were maybe the clumsy kid, always tripping or running into walls and furniture that had been in your house your whole life. For many in this bendy world, diagnosis isn’t able to be made for another 17-22 years (average age of diagnosis is 31!) (Daylor, 2025)
Back then, you were likely able to manage, largely due to high participation in athletics and stable hormone circulation. In your 20s, things may have started to slip, but you hit a major turning point between 30 and 40. Between childbirth, work stress, and the onset of perimenopause, hormone shifts lead to frank dislocations and instabilities.
Suddenly, your body feels a bit more “old” than it should at this point. For many, this leads us to our primary care physician or consulting Dr. Google, only to be told it’s likely just due to stress or perimenopause, and to wait it out. Oftentimes you may get a diagnosis of fibromyalgia or chronic fatigue syndrome, and be left with loose ends with a diagnosis that covers some of your symptoms but not all.
Medical Gaslighting
You go to the doctor asking the hard questions:
- “Why am I tired all the time?”
- “Why can’t I lift my children?”
- “Why is my SIJ out of place?”
Only to be told it’s just part of being a woman. You’re told you’re just “weak” or that you’re “tight” and should stretch. Worse yet, maybe you start a stretching program or regular yoga and find that symptoms get worse instead of better.
You get told that despite feeling your joints click, clunk, and shift, that you can’t be dislocating because you don’t have a history of traumatic injury. If you’re lucky, you’ll get an umbrella diagnosis like fibromyalgia, chronic fatigue syndrome, IBS, or pelvic floor dysfunction.
The medical world collectively gives you a shrug and says, “Deal with it, it’s perimenopause, baby” and yet, you go home with more questions than you went in with.
In May of 2025, a retrospective study found of 425 patients diagnosed with EDS, 405 of them (94.4% of the total study population, which was already 95% female) had reported that they experienced medical misdiagnosis including the potential of getting told “it’s all in your head”. (Lee 2025).
I am here to tell you, its NOT all in your head. There may be a link to all of these symptoms, and an experienced professional who will evaluate all of your symptoms can help.
Self advocacy is so incredibly important to getting your answers. Finding medical professionals that will sit with you and hear ALL of your symptoms and look for the common cause are also vital. For those on the hypermobile spectrum, support groups in your area, or searching the Ehlers Danlos Society website can help you find professionals who are experts in treating hypermobility, and can help manage your symptoms and pursue formal diagnoses.

Understanding the “Why”: Collagen and Systems
What is actually happening? Hypermobility is a connective tissue disorder affecting collagen proteins. We used to think it only meant “bendy joints,” but collagen is in every system of the body. This is why you experience:
- Proprioception issues: A struggle to detect where you are in space (the clumsiness).
- Interoception issues: Not feeling internal signals (hunger, thirst, needing to pee) until it’s an emergency. This is why you may not feel an injury until hours later.
- Systemic symptoms: TMJ, migraines, GI dysfunction, and even pelvic floor issues (leaking or pain). Up to 99.4% of HSD/hEDS patients surveyed in a 2025 study (Daylor 2025) cited dysautonomia symptoms. It’s virtually a guarantee that hypermobile bodies will have some degree of dysautonomic symptoms .
- The Neurodivergence Link: A surprising correlation between hypermobility and Autism or ADHD. When surveying the rates of systemic joint hypermobility in neurotypical vs neuro divergent groups, hypermobility was roughly 4 times as prevalent in a patient with confirmed diagnosis of neurodivergence. (Csecs 2022)
- Hormonal Impact: Estrogen stimulates collagen production and maintains bone density. As levels shift in your 30s and 40s, the “glue” holding you together weakens.
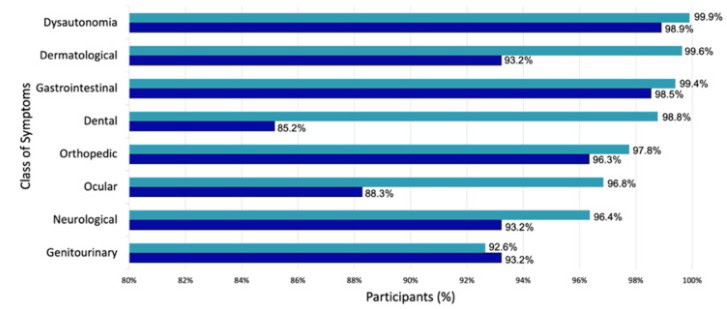
The above graph was from a 2025 global survey of people with Hypermobility Spectrum Disorders and Hypermobile Ehlers Danlos Syndrome, and it shows the most commonly reported symptoms tied to hypermobility. If you feel like everything is seemingly related to hypermobility, it is. Connective tissue is everywhere.
The Physical Toll of Daily Life
Now, your kids are getting older and faster. You want to keep up with them, but you can’t without feeling aches for days. If you overdo it, you need four business days in bed to recover. However there are still things to do, so you have to push through to cook and clean, making the problem worse.
The fatigue that s-hEDS patients experience is related to multiple factors; both from the condition itself and as a by-product of the medications prescribed to manage it. With dysautonomia/POTS, quick changes in position, internal pressure, or stress can cause rapid changes to blood pressure or heart rate, causing that near-faint feeling. We also get muscle fatigue from constantly working to help stabilize the joints that lax ligaments can’t.
Sleep disturbances from high sympathetic nervous system activity (fight or flight) and sleep apnea can prevent proper restorative sleep at night. Even at the cellular level, the powerhouse of the cell, the mitochondria, have been found to have dysfunctional patterns of synthesizing cellular energy. All of this, on top of regular life stressors increases the fatigue. The more you push through the worse it gets. (Chopra 2025)
You find yourself leaning on everything: grocery carts, walls, counters. You rest your head in your hands, jut your hip out, and cross your legs all the way around just to feel “held.” People ask, “Are you sure you’re comfortable like that?” but those weird positions are the only way to quiet your brain. They feel restorative. You’d rather sit on the floor than in a chair. You enter a cycle of sleep aids to pass out, stimulants to stay awake, and every supplement in the vitamin aisle, yet nothing seems to help.
The S-hEDS lean, and requiring floor time to focus or recover from the day is extremely common. We do this because the brain has a hard time with proprioception, the sense of position in space, as well as an internal cue of lacking stability. When the perceived instability combines with chronic pain, chronic fatigue, and reduced muscle control, finding support on external objects is comforting to the nervous system, and is a subconscious method of reducing injury risk. (Bates, 2021)

The Path Forward: How to Manage “Falling Apart”
If you go to a standard PT, they might tell you to stretch. You try it, and things feel worse. Instead, look back at high school: when you were active and strong, your muscles held your joints together.
Step 1: Get Strong (and Stay Strong)
Muscles are your internal bracing system. Working with a trainer or PT who understands hypermobility is imperative. While it has been found that those within the hypermobile community often are noted as weaker than age- and gender-matched peers, (Rombout) muscle mass was not different, and didn’t contribute to strength deficits. It is then theorized that the differences in strength are more related to the presence of pain and fatigue in the hEDS/HSD world. Ferrell et al in 2004 found that a regular exercise program improved strength in the legs and balance, as well as symptoms of proprioception, chronic pain and quality of life and physical function. Bathen et al (2013) echoed these findings that a programmed regular exercise program improved self reported participation in daily life, strength and endurance as well as a significant reduction in kinesiophobia (fear of movement)
Some of my favorite hEDS/HSD resources for training and understanding on instagram are:
- @hypermobile.work (also on YouTube!)
- @hyperresilient
- @growwithmenatalie
- @doc_ashtonn
- @dr.melissakoehl.pt
- @hypermobilityhealthcoach
- @Kim_moscatello
- @thenorrislab
- Or, you can find ME @Gallagher.DPTSCS
Step 2: Use Your Tools
On flare days, use the braces, taping, and splints. They aren’t “crutches”; they are tools to help you participate in life.
Here’s a link (not sponsored) for helpful hEDS/HSD aides and braces.
Step 3: Monitor Your Energy
Use the “Gas Tank” comparison. If making breakfast takes half a tank, you need to adjust your day. Don’t wait until you’re on “E” to rest.
Energy conservation and management throughout your day is a key way to make sure we get to the end of the day without crashes.
Sometimes, this means prioritizing some tasks and delaying others. One thought framework is imagining all of the things on your to-do list as glass balls or rubber balls.
The glass balls are the things that need to get done: eating regular meals, personal hygiene, and often tasks for work near their deadline. Rubber balls are the things that can be put off until a higher energy day: putting away the laundry, emptying the dishwasher (when there are clean dishes available to use).
Step 4: PT and Regenerative Medicine
Use a trusted PT as your first line of defense for subluxations. If things are more serious or uncontrollable instability, maybe consider PRP or prolotherapy, then as a last resort, surgery. In a literature review by Svensden et al in 2025, they found that for shoulders, hips, knees and elbows, orthopedic surgical outcomes were similar, or slightly worse, in hypermobile patients when compared to non-hypermobile cohorts. For the ankle however, hypermobile people were consistently found with more recurrent instability and worse outcomes. They also found that when hypermobile individuals went under FAI/labral repair in the hip they were more likely to develop post-operative iliopsoas tendonitis (hip flexor tendonitis).
As far as ACLs (knee) are concerned, there was only a very slight indication of higher re-tear rates in hypermobile patients, with those with higher Beighton scores and increased laxity in the thumb, pinky and knee hyperextension increased the likelihood of ACL re-tears. While some of these results may suggest influence on clinical decision making, proceed with caution: the studies included had LARGE variation in what they determined “hypermobile” (4/9 vs 7/9 Beighton) and was a very mixed population that may have overdiagnosed generalized joint laxity. As always in the hypermobile world, more research is needed.
References/Sources
- Bates AV, McGregor AH, Alexander CM. Prolonged standing behaviour in people with joint hypermobility syndrome. BMC Musculoskelet Disord. 2021 Dec 1;22(1):1005. doi: 10.1186/s12891-021-04744-1. PMID: 34852804; PMCID: PMC8638551.
- Bathen T, Hångmann AB, Hoff M, Andersen LØ, Rand-Hendriksen S. 2013. Multidisciplinary treatment of disability in Ehlers–Danlos syndrome hypermobility type/hypermobility syndrome: A pilot study using a combination of physical and cognitive-behavioral therapy on 12 women. Am J Med Genet Part A. 161A: 3005–3011
- Chopra, P. (2025, March 16). Fatigue in Ehlers-Danlos Syndrome (EDS). https://www.painri.com/post/fatigue-ehlers-danlos-syndrome-eds
- Csecs JLL, Iodice V, Rae CL, Brooke A, Simmons R, Quadt L, Savage GK, Dowell NG, Prowse F, Themelis K, Mathias CJ, Critchley HD, Eccles JA. Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Front Psychiatry. 2022 Feb 2;12:786916. doi: 10.3389/fpsyt.2021.786916. PMID: 35185636; PMCID: PMC8847158.
- Daylor V, Griggs M, Weintraub A, Byrd R, Petrucci T, Huff M, Byerly K, Fenner R, Severance S, Griggs C, Sharma A, Atwal P, Kautz SA, Shapiro S, Youkhana K, Lavallee M, Wilkerson A, Nichols M, Snyder A, Eichinger JK, Patel S, Maitland A, Gensemer C, Norris RA. Defining the Chronic Complexities of hEDS and HSD: A Global Survey of Diagnostic Challenges, Life-Long Comorbidities, and Unmet Needs. J Clin Med. 2025 Aug 9;14(16):5636. doi: 10.3390/jcm14165636. PMID: 40869462; PMCID: PMC12386360.
- Ferrell, W.R., Tennant, N., Sturrock, R.D., Ashton, L., Creed, G., Brydson, G. and Rafferty, D. (2004), Amelioration of symptoms by enhancement of proprioception in patients with joint hypermobility syndrome. Arthritis & Rheumatism, 50: 3323-3328. https://doi.org/10.1002/art.20582
- Lee C, Chopra P. The Incidence of Misdiagnosis in Patients with Ehlers-Danlos Syndrome. Children (Basel). 2025 May 29;12(6):698. doi: 10.3390/children12060698. PMID: 40564656; PMCID: PMC12191865.
- Svendsen C, Vivekanantha P, Braunstein D, Raja S, Jagdeo V, Duong A, Simunovic N, Ayeni OR. Outcomes after Surgical Management of Large Joint Manifestations in Ehlers Danlos Syndrome and Hypermobility Conditions in Sports Medicine: a Systematic Review. Curr Rev Musculoskelet Med. 2025 Oct;18(10):429-459. doi: 10.1007/s12178-025-09979-2. Epub 2025 May 21. PMID: 40397373; PMCID: PMC12325825.
About the Author

Dr. Colleen Gallagher is a Board-Certified Sports Clinical Specialist and physical therapist based in Northern Virginia. She specializes in sports performance for weightlifters, runners, and overhead athletes, while also providing expert care for postpartum athletes, hypermobility conditions (EDS/HSD), and pediatric patients. As an eating disorder-aware clinician, Dr. Colleen prioritizes a health-first, body-neutral approach focused on function, resilience, and sustainable progress. Her mission is to empower motivated individuals to safely train, prevent future injuries, and confidently return to the activities they love.
Share This Page
Related Resources
Found this page interesting? Discover more insightful resources below.





