I’ll confess something: one of my favorite ways to spend a free hour is watching pitchers in high-quality slow motion. Not Bridgerton (mostly my wife… mostly). Not Stranger Things (too dark). A 100-mph fastball broken down frame by frame, looking for the thing that makes a shoulder last… or the thing that eventually breaks it.
After years of doing this, one muscle keeps pulling my attention: the subscapularis.
It doesn’t get the press of the supraspinatus or infraspinatus (posterior cuff). Nobody writes dramatic injury headlines about it. But the subscapularis is the largest and most powerful muscle in the rotator cuff, responsible for roughly 53% of total cuff strength. And for pitchers, it may be the most important one to understand, train, and protect.
Here’s why.
What Happens to the Subscapularis When You Pitch
To understand the demand, you need to understand the moment.
Late cocking (what coaches call “layback”) is the phase where the throwing arm reaches maximum external rotation before the shoulder whips forward into acceleration. It’s one of the most extreme positions the human body produces voluntarily, and it’s also where the subscapularis is most vulnerable.
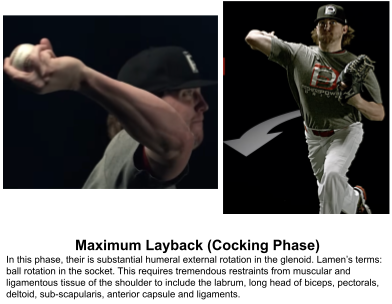
During this phase, the anterior shoulder absorbs a compressive and distractive load estimated at 50–100% of body weight. For a 200-pound pitcher, that’s up to 200 pounds of force on a single shoulder, in an end-range position, generated in a fraction of a second. The cocking phase (from front leg raise to ball release) also represents roughly 80% of the total pitching motion by duration. That means the subscapularis isn’t just working hard. It’s working hard for a long time, relative to everything else happening in the throw.
EMG research confirms what the physics suggests: the subscapularis shows the highest muscle activation of any rotator cuff muscle during late cocking. It’s the primary restraint against unchecked external rotation and anterior humeral head translation. When it’s delayed, inhibited, or injured, the joint loses centration, and other structures start absorbing load they weren’t designed to handle.
This is not a muscle you can afford to ignore.
Two Things to Check Before You Train It
Before loading the subscapularis, assess it. Two things matter most: range of motion and strength. Think of these as your baseline before programming anything.
Range of Motion
Adequate shoulder external rotation is what creates the “window” for energy transfer during the pitch. Without it, pitchers compensate by finding velocity through the elbow, spine, or hips instead of the shoulder. That compensation is where injuries begin.
How to measure it:
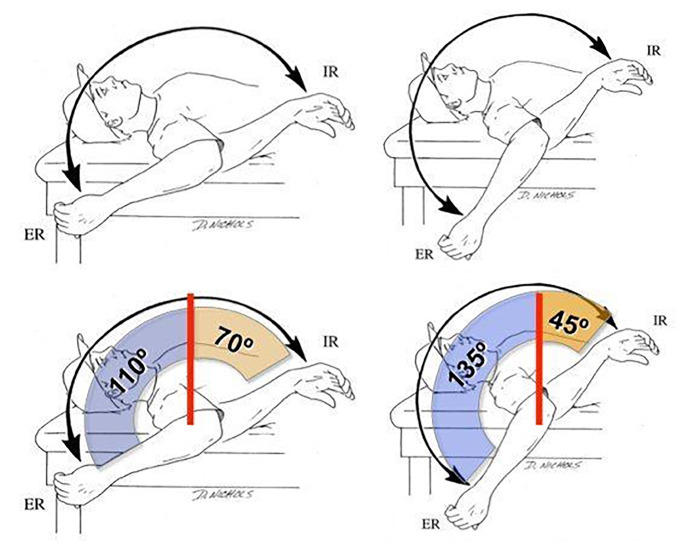
Position the athlete so the scapula is stabilized and the trunk can’t cheat with rotation or extension. Measure external rotation (ER) with a goniometer or a smartphone inclinometer app. Most healthy throwers show 100–120° of ER in the throwing shoulder at 90° of abduction.
The number that actually matters most, though, is total arc of motion: the sum of internal rotation (IR) and external rotation (ER) in the same position.
Research is clear on this: pitchers with a total arc below 160° are at significantly higher risk of shoulder injury, and those with limited total arc have been shown to undergo overstretching toward ER during late cocking, thereby placing greater load on the anterior structures, including the subscapularis. Pitchers with adequate total arc can throw just as hard without the same upper extremity loading.
Practical thresholds:
- Total arc below 180°: worth monitoring
- Total arc below 160°: mobility work is indicated
- ER below 100° with total arc below 160°: prioritize targeted mobility work (stretching, soft tissue work, dynamic mobility)
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC7872440
When to stop and get evaluated
If the pitcher has pain, feelings of instability or giving way, or stiffness that doesn’t respond to mobility work after 1-2 weeks, that’s a referral. A proper evaluation should include both a structural diagnosis (subscapularis tear, labral injury, biceps pathology) and a movement-based diagnosis (scapular control, thoracic mobility, lat and pec length and strength, rotator cuff strength ratios, etc.). A structural and a movement-based diagnosis are not the same thing, and injured pitchers need both.
Strength
Once you’ve confirmed the tissue can tolerate load, test it.
A simple starting screen is the belly press test or bear hug test. Both produce high subscapularis activation while keeping other internal rotators relatively quiet (pectoralis major, latissimus dorsi, teres major, and anterior deltoid).
Research shows the bear hug test has the highest sensitivity of the common subscapularis clinical tests (up to 55–74% depending on the study), with specificity above 90% for both.
Neither test is perfect. False positives exist, and isolated subscapularis tears are notoriously difficult to catch clinically, but pain or notable side-to-side weakness during either test warrants a baseball-informed medical evaluation before loading the shoulder further.
If you have access to isometric strength testing, measure:
- Max isometric internal rotation (IR)
- Max isometric external rotation (ER)
- The ER:IR ratio
A commonly cited target for the ER:IR ratio is 2/3 to 3/4 (66-75%). A ratio closer to 1:1 can indicate either unusually strong external rotators or relatively weak internal rotators, either of which may reflect a glenohumeral stability issue worth addressing.
For IR strength benchmarks, normative data for pitchers suggests:
- IR at 90° abduction: approximately 20–25% of bodyweight (40–50 lbs for a 200-lb pitcher)
- IR at the side: approximately 10–15% of bodyweight (20–30 lbs for a 200-lb pitcher)
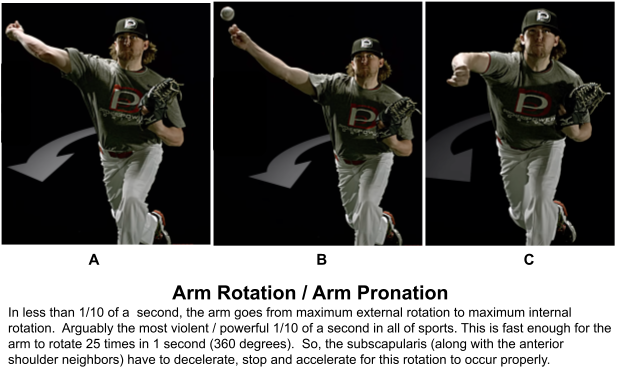
One important nuance: strength is not the same as rate of force development. Most athletic movements (including the pitching delivery) happen in the blink of an eye (30–200ms).
The ACL tears in 30ms. The shoulder reaches maximum external rotation in a similarly brief window.
An athlete can test at near-normal max strength and still have significant deficits in how quickly they can produce that force. Isometric testing captures max output; it doesn’t fully capture the explosive demand of throwing. Keep that in mind when interpreting results and programming.
A cable machine with constant weight and rep comparisons side-to-side is more of an endurance measure. It’s less reliable and doesn’t map well to the max output demands of throwing. Isometric testing, or a functional trainer that can measure power output, is more appropriate for this population, which I have in my clinic.
One Warning Sign Coaches and Parents Should Know
An unexplained drop in velocity or command is not just a performance issue. Research published in 2022 found that loss of 4-seam fastball command (specifically, more elevated and out-of-zone pitches) was objectively associated with impending shoulder injury in MLB pitchers in the month before they were placed on the injured list. The authors noted that command loss may be an early indicator of altered kinematics or shoulder injury before pain even presents.
In plain terms: if a pitcher’s location or velocity drops without an obvious explanation, screen ROM and strength before assuming it’s mechanical or mental. It may be neither.
This requires coaches, athletes, and parents to communicate openly and without stigma.
The Bigger Picture: Arm Care
The subscapularis doesn’t exist in isolation. Protecting it means protecting the whole system.
Real arm care is not a band exercise circuit. It’s the full stack: sleep and nutrition, warm-up and movement prep, workload management (pitch/long toss counts matter tremendously), strength and conditioning of the upper extremity and the lower half, mobility work, and honest conversations about velocity-at-all-costs training culture.
One finding worth highlighting for coaches: a 2021 prospective study found that ankle dorsiflexion deficit in the back (drive) leg was a significant independent risk factor for shoulder and elbow injuries in young pitchers. The kinetic chain runs from the ground up. A stiff ankle on the push-off leg changes how force is transferred through the hips, trunk, and eventually the shoulder. This is why I’m equally obsessed with the foot and ankle — and why more on that is coming in a future post.
For a relatively comprehensive arm care framework, Mike Reinold and Champion Physical Therapy and Performance remain among the most credible resources in the field. It’s part of why I pursued the Baseball Rehabilitation Specialist certification through Champion, even after directing an upper extremity athlete fellowship program, pitching in college, and running an adult baseball league for over 20 years.
The field keeps moving. So should we.
When to See a Baseball-Informed Provider
Not every shoulder issue needs a medical evaluation. But some do, and the distinction matters.
Get evaluated if:
- There is pain during or after throwing that doesn’t resolve with rest
- ROM or strength shows significant asymmetry that doesn’t respond to training
- Velocity or command drops without explanation
- There are feelings of instability, catching, or giving way
The right provider is a DPT, ATC, or sports medicine physician with baseball-specific experience.
A physical therapist can also determine whether and how urgently a sports medicine physician consultation is needed. The goal of that first visit is usually clarity; ruling out serious structural pathology, identifying movement deficits, and building a personalized plan.

Want a Personalized Plan?
If you or a pitcher you know wants individualized guidance, contact me or another MovementX provider here.
Options include:
- Free 20-minute call to talk through your situation
- 90-minute evaluation with advanced testing and a clear plan
- 30-minute in-person screening
Happy pitching, fellow simians.
References
- Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparative electromyographic analysis of the shoulder during pitching: professional versus amateur pitchers. Am J Sports Med. 1987;15(6):586–590. doi:10.1177/036354658701500611
- Schofield MR, Paul RW, Buchheit P, Rauch J, Thomas SJ. Chronic adaptation of the coracohumeral space and subscapularis tendon in professional baseball pitchers. Sports Health. 2025;17(4):752–758. doi:10.1177/19417381241270359
- Itoi E, et al. Limited total arc glenohumeral rotation and shoulder biomechanics during baseball pitching. J Athl Train. 2024;59(10):997–1003. doi:10.4085/1062-6050-0565.23
- Paul RW, et al. Chronic adaptations of the shoulder in baseball pitchers: a systematic review. Am J Sports Med. 2025. doi:10.1177/03635465251317202
- Kappe T, et al. Diagnostic accuracy of clinical tests for subscapularis tears. Orthop J Sports Med. 2022;10(2). doi:10.1177/23259671221074783
- Barth JR, Burkhart SS, De Beer JF. The bear-hug test: a new and sensitive test for diagnosing a subscapularis tear. Arthroscopy. 2006;22(10):1076–1084.
- Nakaji RM, Ellenbecker TS, et al. Descriptive strength and range of motion in youth baseball players. Int J Sports Phys Ther. 2021;16(1):93–103. doi:10.26603/001c.18815
- Tanaka H, et al. Ankle dorsiflexion deficit in the back leg is a risk factor for shoulder and elbow injuries in young baseball players. Sci Rep. 2021;11(1):5500. doi:10.1038/s41598-021-85079-8
- Glanzer JA, et al. More elevated fastballs associated with placement on the injured list for shoulder injuries in Major League Baseball pitchers. Orthop J Sports Med. 2022;10(5). doi:10.1177/23259671221094098
- Oeding JF, Boos AM, Kalk JR, et al. Pitch-tracking metrics as a predictor of future shoulder and elbow injuries in Major League Baseball pitchers: a machine-learning and game-theory based analysis. Orthop J Sports Med. 2024;12(9). doi:10.1177/23259671241264260
- Caplan N, et al. The early cocking phase and upper extremity surgery risk in starting professional baseball pitchers. Am J Sports Med. 2015;43(10). doi:10.1177/0363546515602016
About the Author

Dr. Kris Porter is a Board Certified Orthopedic Clinical Specialist, Baseball Rehab Specialist, and physical therapist in Northern Virginia. Dr. Kris is passionate about delivering value-driven care through the minimum effective dose, ensuring that every session is optimized for efficiency and real-world results. His goal is to respect your time while empowering you to overcome injury, improve performance, and return to the activities that bring you joy.
Share This Page
Related Resources
Found this page interesting? Discover more insightful resources below.





